Injured in Ontario? Get clear legal guidance today.
Our personal injury team can help with accident, disability, and injury claims. Contact us today for a free consultation.

In an Ontario personal injury claim, medical records often become the timeline insurers and defence lawyers rely on most.
Strong documentation connects your symptoms, treatment, work restrictions, and daily-life impact over time. Weak or inconsistent records can create avoidable problems even when your injury is real.
After a car accident, a slip and fall, or any injury caused by someone else’s negligence, the standard advice is immediate: see a doctor. That advice is correct. But the part that is less often explained is that it is not just the visit that matters — it is what gets written down, when, and how it connects to your claim over time.
Your medical records function as a real-time timeline that insurers and defence lawyers will examine carefully. A well-documented chart makes a claim easier to support. A chart with gaps, vague entries, or accidental inconsistencies gives the other side a tool to use against you — even when every word you have said about your injury is completely true.
This guide covers what makes medical documentation strong in an Ontario personal injury claim, what common patterns create problems, and what you can do at your appointments without turning every visit into a legal exercise.
In a personal injury claim, insurers are not assessing your pain the way your family does. They are assessing proof — specifically, contemporaneous written evidence created close in time to the incident by qualified health professionals. That evidence is treated as more reliable than anything you say months or years later.
Your medical chart answers questions that are central to every injury claim: Did you report symptoms promptly, or did you wait? Did symptoms progress in a way that makes medical sense? Did you follow through on treatment? Were there unexplained gaps in care? Did you describe your condition consistently across providers? Did anyone document how the injury changed your daily functioning?
A consistent, coherent medical timeline makes a claim more defensible. A fragmented or contradictory one raises credibility questions — particularly in claims involving soft tissue injuries, concussion, chronic pain, psychological injuries, or any condition that does not appear clearly on imaging. These are exactly the injuries where the written record becomes most important, because there is no visible fracture to point to.
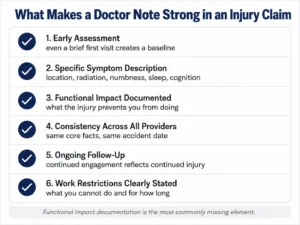
Adrenaline after an accident can mask pain temporarily. Many injuries — particularly soft tissue and neurological — worsen over the days following the incident. Getting assessed early, even at a walk-in clinic or urgent care, establishes a baseline and defeats the insurer’s common argument that a delay in seeking treatment means the injury was not serious or was caused by something else. Even a brief initial note with a date and initial complaint creates a starting point that is very difficult to argue against later.
“Pain” alone is too vague to support a strong claim. The details that translate well into documentation include the precise location of pain, whether pain radiates and where, the presence of numbness or tingling, headaches, dizziness, nausea, sleep disruption, and cognitive symptoms such as difficulty concentrating or memory problems. Psychological symptoms — anxiety in vehicles, nightmares, panic — are also important to report and document. You do not need medical terminology; your provider will translate your description into clinical language. The key is specificity.
One of the most important distinctions in personal injury documentation is the difference between symptoms and functional impact. A note that says “back pain” is weaker than a note that says “patient cannot sit for more than 20 minutes without pain, required to stand and stretch repeatedly, currently unable to perform job duties.” The damages in a personal injury claim are about how the injury changed your life — and the medical record is where that change should be documented.
Relevant functional details include difficulty lifting, inability to perform specific work tasks, missed shifts, driving limitations, trouble with stairs, disrupted sleep, and inability to participate in activities you did before the accident. Your pain and suffering valuation is directly affected by how well this functional impact is captured in the medical record. Our guide on how much pain and suffering is worth in Ontario explains how courts assess this in more detail.
You may see a family doctor, physiotherapist, chiropractor, massage therapist, psychologist, and one or more specialists over the course of your recovery. The core facts of your case need to remain consistent across all of these records — the accident date, the mechanism of injury, the main areas of complaint, and the general progression of symptoms. Symptom variation is normal and expected; the fundamental facts should not shift. When the story changes across providers without explanation, insurers treat it as a credibility problem.
Frequent follow-up is not about optics — it is about health. But it also builds a coherent medical timeline. If symptoms persist, continuing to see providers, asking for referrals when progress stalls, and keeping the clinical loop active creates a record that reflects ongoing injury rather than a one-time event that resolved. In terms of your claim, a chart showing continued clinical engagement is significantly more useful than a chart that shows one or two early visits and then nothing for months.
If you cannot work or require modified duties, that needs to be clearly documented in the clinical record — what you cannot do, any applicable weight limits or positional restrictions, how long restrictions are expected to apply, and when reassessment is scheduled. This documentation is essential for income replacement benefit claims under Ontario’s SABS accident benefits system and for wage loss claims in tort.

Many people downplay how they feel in the emergency room or at their first visit — “I’m okay, just shaken up” — either because adrenaline is still masking the injury or because they do not want to seem dramatic. That initial minimization becomes part of the permanent record. If you subsequently report significant symptoms, the early “I’m fine” note will be used to argue that the injury either did not occur as described or developed from a different cause. If you have any pain, stiffness, or discomfort at your first assessment, report it accurately even if it feels mild.
People stop or pause treatment for legitimate reasons: cost, work schedule constraints, transportation barriers, childcare, waiting for benefit approvals, or mental health capacity. Insurers consistently interpret unexplained gaps as evidence of recovery. The gap itself is not automatically fatal to a claim — the absence of documentation explaining the gap is what creates the problem. When you return to care after an interruption, explain why you were away. If the barrier is noted in the clinical record, it reads very differently from a gap with no explanation. Insurers also use surveillance around periods of treatment gaps to try to establish that the claimant was more active than reported during the pause.
Casual comments about other physical activities can permanently complicate a claim. If you mention to a provider that you were sore after helping someone move, or that you have been doing home renovations, and your primary injury is from the accident, that comment may appear in the chart in a way that defence lawyers will later argue explains your pain. Be precise and careful about how you describe any other activities or physical demands. If you have a pre-existing condition, that does not eliminate your claim — in Ontario, an accident that aggravates a pre-existing condition is still compensable — but the clinical record needs to reflect clearly what your baseline was before the accident and how the accident changed it.
Repeated missed appointments, stopping treatment without explanation, declining recommended investigations, or not taking prescribed medications can all generate language in your chart — “non-compliant,” “missed appointment,” “declined referral” — that insurers use to argue you were not committed to recovery. If you cannot comply with a recommendation for a legitimate reason, document that reason with your provider and ask for alternatives. There is a significant difference in the record between “patient declined physiotherapy” and “patient unable to attend physiotherapy due to financial barriers — exploring covered alternatives.”
Some clinics produce standardized notes that look the same at every visit — the same boilerplate language, no documented change in function or symptoms, no measurable findings. These records establish attendance but do not build a clinical picture. If one provider is producing thin documentation, the detailed notes from another treating professional carry more weight. A well-documented physiotherapy or psychological record can compensate for a sparse family doctor chart in some cases.
Pain severity ratings can vary legitimately between visits — that reflects the variable nature of many injuries. But large inconsistencies without explanation create credibility problems. Reporting a pain level of 9 out of 10 with one provider and 2 out of 10 with another, without documentation of why the gap exists, will be used against you. The solution is not to flatten your reporting — it is to be specific about variability. “Pain fluctuates between 2 and 8 depending on activity” is accurate and defensible. An unexplained 7-point swing between two records is not.
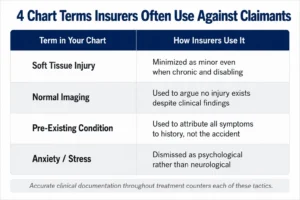
This phrase sounds minor to non-medical readers. Insurers rely on that perception. Whiplash and soft tissue injuries in Ontario can be severe and chronic, but the ongoing documentation needs to reflect persistence, functional limitation, and any objective clinical findings to counter the insurer’s minimization of the diagnosis label.
Normal X-rays or MRI results mean no structural damage was detected — they do not mean no injury exists. Many significant injuries produce normal imaging results. Clinical examination findings, documented functional limitations, and symptom history carry the evidentiary weight in these cases. The clinical note, not the imaging report, becomes the primary record.
A pre-existing condition does not eliminate a claim in Ontario. An accident that aggravated or accelerated a pre-existing condition creates a compensable injury. The clinical record needs to document your baseline before the accident and the change that followed. Without that documentation, the pre-existing condition becomes a tool for the defence to argue the accident caused nothing new.
Psychological injuries are real, recognized, and compensable in Ontario personal injury claims. PTSD, depression, driving anxiety, panic disorder, and chronic sleep disruption are all consequences of serious accidents that have been successfully included in claims. If you are experiencing psychological symptoms, report them to your healthcare provider, ask for a referral to an appropriate mental health professional, and ensure they are documented from early in your treatment history.
You do not need to turn every medical appointment into a legal strategy session. A few straightforward habits protect your documentation without being artificial.
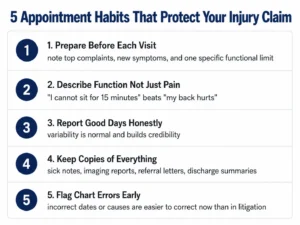
Before each visit, take two minutes to note your top two or three current complaints, any new symptoms since the last visit, what has improved and what has worsened, and at least one specific daily activity that your injury is currently preventing or limiting. This prevents the common situation of arriving at an appointment, being asked “how are you?” and responding “fine” because you are managing in the moment.
Describe your limitations in functional terms rather than abstract pain levels. “My back prevents me from sitting at a desk for more than 15 minutes” is more useful documentation than “my back hurts a lot.” Describe what the injury does to your day.
Be honest about good days. Reporting improvement when it occurs makes you more credible, not less — it shows normal recovery variability rather than a fixed narrative. If progress has stalled, say that too, and ask what the next step is.
Keep copies of what you receive — sick notes, specialist reports, imaging results, discharge instructions, and referral letters. Your lawyer can request full records later, but having your own file reduces the risk that something is missed or lost.
If something in the chart is recorded incorrectly — a wrong accident date, a symptom attributed to the wrong cause — address it at your next visit by politely asking the provider to clarify or amend the record. Errors caught early are far easier to manage than errors that are not discovered until litigation.
Common insurer review points include:
Understanding these patterns lets you avoid inadvertently creating problems without exaggerating or misrepresenting anything. Our post on why not to accept the first insurance offer covers the broader context of how insurers use the file in settlement negotiations.
A messy medical file is common. People are injured, stressed, managing work and family obligations simultaneously, and often do not realize the clinical record will matter until much later in the process. The right response to imperfect documentation is not panic — it is action.
If symptoms persist, return to care and be specific about what is still going on and how it is affecting your daily life. If progress has stalled, ask for referrals to specialists or allied health professionals. If treatment gaps exist without documented explanations, address those gaps in clinical notes going forward. And get legal advice — both to understand what your current documentation means for your claim and to ensure you do not inadvertently make things worse through the claims process itself.
In Ontario, personal injury claims are subject to a two-year limitation period. Getting advice while time remains is significantly better than waiting until the medical record has been frozen by time and the claim has become more difficult to pursue.
Related reading:
Seeking medical attention as early as possible is strongly advisable, but it is not technically a legal requirement for filing a claim. The practical problem with delay is that it gives insurers and defence counsel an argument that the injury was not serious, or that something else caused your symptoms. Even a brief initial assessment at a walk-in clinic shortly after the accident creates a baseline that is difficult to challenge later.
Normal CT or MRI results do not mean no injury exists. Many injuries — including soft tissue damage, concussion, and nerve irritation — do not appear on standard imaging. The clinical examination findings documented by your healthcare providers, combined with consistent reporting of functional limitations across visits, carry the evidentiary weight in these cases. Do not assume a normal imaging result ends your claim.
No. In Ontario, an accident that aggravates, accelerates, or worsens a pre-existing condition creates a compensable injury. The clinical record needs to document your pre-accident baseline and the change that followed the accident. A personal injury lawyer can help ensure this is properly framed in the context of your claim.
Raise the issue with your healthcare provider at your next visit and ask them to clarify or correct the record. Providers do make documentation errors — a wrong date, a symptom attributed to the wrong cause, a misunderstood complaint. Errors caught and corrected early in the process are significantly easier to manage than errors discovered during litigation. If the correction is contentious or involves something material to your claim, get legal advice before approaching the provider.
Yes. Psychological injuries are recognized and compensable in Ontario personal injury claims. PTSD, depression, driving anxiety, panic disorder, and sleep disruption are all consequences of serious accidents that courts and insurer systems recognize. If you are experiencing these symptoms, report them to your healthcare provider early, ask for a referral if appropriate, and ensure they appear consistently in your clinical record.
Unexplained gaps in treatment are one of the most common tools insurers use to argue that a claimant recovered during the gap period. The gap itself is not automatically fatal — the absence of a documented explanation is what creates the problem. If your treatment was interrupted for a legitimate reason, ensure that reason is noted in the clinical record. When you return to care, explain the context of the gap to your provider and ask that it be recorded.
Our personal injury team can help with accident, disability, and injury claims. Contact us today for a free consultation.


